| Species | Tier | Onset | Key Action |
|---|---|---|---|
| Galerina marginata | Tier 1 | 6–24 hr | Immediate hospitalization, hepatic panels, Silibinin/NAC |
| Amanita bisporigera | Tier 1 | 6–24 hr | Immediate hospitalization, hepatic panels, Silibinin/NAC |
| Amanita arocheae | Tier 1 | 6–24 hr | Immediate hospitalization, hepatic panels, Silibinin/NAC |
| Amanita verna | Tier 1 | 6–24 hr | Immediate hospitalization, hepatic panels, Silibinin/NAC |
| Lepiota cristata | Tier 1 | 6–24 hr | Immediate hospitalization, hepatic panels, Silibinin/NAC |
| Gyromitra infula | Tier 1 | 6–12 hr | IV Pyridoxine 25 mg/kg + anticonvulsants |
| Cortinarius rubellus | Tier 1 | 3–21 days | Nephrology consult, renal replacement therapy |
| Lepiota subincarnata ⚠ | Warning | 6–24 hr | Treat as Tier 1 amatoxin poisoning immediately |
| Inocybe geophylla | Tier 2 | 15–30 min | Atropine (dry secretions only) |
| Clitocybe dealbata | Tier 2 | 15–30 min | Atropine (dry secretions only) |
| Amanita muscaria | Tier 2 | 30 min–2 hr | Supportive care — NO Atropine |
| Chlorophyllum molybdites | Tier 2 | 30 min–3 hr | IV rehydration, electrolytes |
| Macrocybe titans | Tier 3 | 30 min–3 hr | Oral/IV rehydration |
| Psilocybe cubensis | Tier 3 | 30 min–1 hr | Supportive care, benzodiazepines |
▶ Onset-Based Differential Algorithm
🔍 Key Toxidrome Markers
- 🔵 Pinpoint pupils + sweating + slow heart rate = Muscarine → Atropine (to dry secretions)
- 🔴 Delayed severe diarrhea (>6 hrs) + rising liver enzymes = Amatoxin → aggressive hydration + Silibinin/NAC
- 🟠 Delayed neurological changes + seizures (>6 hrs) = Gyromitrin → IV Pyridoxine 25 mg/kg
- 🟡 Polyuria + flank pain, days 3–21 = Orellanine (Cortinarius) → nephrology consult, no antidote
🔴 Life-Threatening Species — Immediate Hospitalization Required
Two major syndromes: Cyclopeptide (Amatoxin) poisoning causing fulminant hepatorenal failure after a 6–24 hour latent period, and Orellanine poisoning causing severe nephrotoxicity with an extraordinarily delayed onset of 3–21 days. Any suspected ingestion of Tier 1 species requires immediate emergency evaluation regardless of symptom absence during the latent phase.
▲ Cyclopeptide Poisoning (Amatoxins) — Amanita bisporigera, Amanita arocheae, Galerina marginata, Lepiota subincarnata
Habitats: high-altitude oak forests of Guatemalan Highlands, Cordillera Central (Costa Rica), Western Highlands of Honduras. Latent period 6–24 hours asymptomatic. GI phase 24–48 hrs: violent cholera-like diarrhea, hematemesis, hypovolemic shock. Apparent recovery 48–72 hrs. Hepatorenal phase 72–96+ hrs: fulminant hepatic necrosis, coagulopathy, encephalopathy, AKI. Mortality >20% without intervention. Treatment: aggressive IV fluids, N-acetylcysteine, IV Silibinin where available, liver transplant evaluation.
▲ Orellanine Poisoning — Cortinarius spp.
Habitats: montane cloud forests of Costa Rica (Chirripó) and Panama, mycorrhizal with native oaks. Latent period 3–21 days. Onset days 3–14: polydipsia, polyuria to oliguria, severe flank pain. Chronic phase: severe acute interstitial nephritis → CKD, hemodialysis or renal transplant. No antidote. Aggressive hydration, nephrology consult.

Deadly Galerina (lookalike)

Deadly Webcap

Destroying Angel (Angel of Death)

Hooded False Morel

Latin American Death Cap

Spring Death Cap

Stinking Dapperling
🟠 Serious — Prompt Clinical Recognition and Treatment Required
Four species across two major syndromes: Gyromitrin poisoning causing refractory seizures requiring IV Pyridoxine, and Muscarine cholinergic syndrome (SLUDGE) requiring targeted Atropine therapy. The Isoxazole syndrome (Amanita muscaria) requires careful differentiation as Atropine is contraindicated unless definitive cholinergic signs coexist.
▲ Gyromitrin Poisoning — Gyromitra infula
Habitats: high-elevation coniferous and mixed forest floors in Guatemala. Latent period 6–12 hrs. Phase 12–24 hrs: headache, vertigo, abdominal cramps, vomiting, diarrhea. Systemic phase 24–48 hrs: pyridoxine depletion → GABA inhibition → refractory fasciculations, delirium, tonic-clonic seizures. Methemoglobinemia, hemolysis, hepatic injury may co-occur. Treatment: IV Pyridoxine hydrochloride 25 mg/kg + anticonvulsant therapy (diazepam).
▲ Muscarine Cholinergic Syndrome — Inocybe geophylla, Clitocybe dealbata
Habitats: ubiquitous — suburban soils, pastures, disturbed forest edges El Salvador to Panama. Hyperacute onset 15–30 minutes: SLUDGE syndrome — Salivation, Lacrimation, Urination, Defecation, GI motility, Emesis. Miosis, bradycardia, bronchospasm. Resolution 2–6 hours. Treatment: Atropine — ceiling note: only to dry secretions, NOT to reverse miosis.

False Parasol

Fly Agaric

Ivory Funnel
White Fiber Cap
🟡 Low Mortality Risk — Supportive Care
GI irritant species causing explosive vomiting and diarrhea, and the Ibotenic Acid / Muscimol isoxazole syndrome. Low direct mortality but significant morbidity from dehydration, particularly in pediatric and elderly patients. Psilocybe cubensis poses significant pediatric risk in cattle-grazing areas.
▲ Severe GI Irritants — Chlorophyllum molybdites
Habitats: manicured lawns, golf courses, parks, pastures — low-to-mid elevation Costa Rica, Nicaragua, Panama. Onset 30 min–3 hours. GI distress 3–8 hrs: explosive vomiting, watery/bloody diarrhea. Resolution 12–24 hrs with rehydration.
▲ Ibotenic Acid / Muscimol Isoxazole Syndrome — Amanita muscaria
Habitats: montane pine forests and introduced exotic timber plots (Guatemala, Honduras). Onset 30 min–2 hrs. CNS phase 2–8 hrs: excitation and depression alternating — visual distortions, ataxia, myoclonus, auditory hallucinations, comatose sleep. Resolution 8–24 hrs. CRITICAL NOTE: Do NOT give Atropine unless definitive severe cholinergic signs coexist.
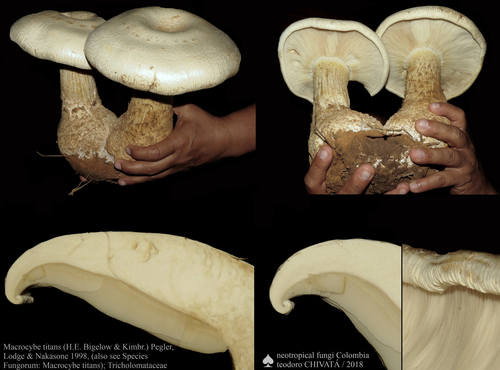
Giant Western Mushroom
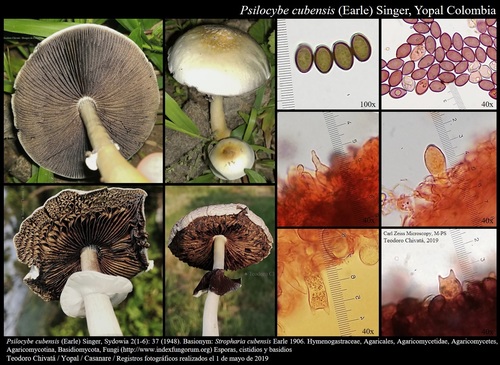
Magic Mushroom
⚠ Misidentification Risk — Treat as Tier 1 on Any Suspected Ingestion
Species that are frequently misidentified as edible and carry life-threatening amatoxin loads. Any suspected ingestion must be treated immediately as Tier 1 poisoning.

Deadly Dapperling
📅 Central America Seasonal Epidemiology
Mushroom fruiting across Central America is driven by altitude and rainfall patterns rather than temperature alone. Key epidemiological patterns for clinicians:
- Rainy season (May–November): Peak fruiting across all elevations. Highest incidence of mushroom poisoning; particularly C. molybdites in lowland suburban areas after heavy rainfall.
- High-altitude Tier 1 risk (Guatemala, Costa Rica, Honduras): Amanita and Galerina species peak during wet season in cloud forests and oak highlands. Subsistence foraging communities face highest risk.
- Orellanine (Cortinarius) late-presentation risk: The 3–21 day latency means patients may not associate renal failure with mushroom ingestion weeks prior. Always take dietary history in unexplained AKI.
- Pediatric risk: P. cubensis in cattle pastures and C. molybdites on suburban lawns represent the primary accidental pediatric exposure risk throughout the region.
- Tourist / visitor risk: Ecotourists in Monteverde, Chirripó, and Guatemalan cloud forests may encounter Tier 1 species; unfamiliarity with regional mycology elevates risk.
- Misidentification risk: C. molybdites is frequently collected as the edible parasol (Macrolepiota procera) — green spore print is diagnostic but often not checked until after ingestion.
🇬🇹 Guatemala
🇨🇷 Costa Rica
Regional Toxicology Note
Central America lacks a standalone region-wide Poison Control Center. Toxicology is managed through regional university public hospitals (Hospital Escuela / Hospital Universitario). Recommended actions: (1) Call country ambulance or Red Cross line for transport to nearest teaching hospital. (2) Photograph mushroom caps, gills, stems, and base if safely accessible. (3) Document exact ingestion-to-symptom timeline for the receiving physician — this is critical for differential diagnosis, especially given the varying latency periods across toxin syndromes.